Using gender/sex information to make clinical decisions: How, why, and with what consequences?
Clinicians regularly apply clinical algorithms to inform decisions about patient care. These tools use patient information as inputs to help assess risk, rule out diagnoses, formulate prognoses, and select approaches to medical and surgical management. Many clinical algorithms ask health care providers to include patients’ gender/sex-related information, most commonly in the form of gender/sex identity markers (i.e., woman/female vs. man/male) and sometimes in the form of sex-linked biological characteristics related to anatomy, pregnancy, menopause, or the use of exogenous estrogenic hormones like oral contraceptives.
In a peer-reviewed paper recently published in Health Affairs, members of the GenderSci Lab collaborated with colleagues at the Harvard School of Public Health, Harvard Medical School, Harvard Law School, Harvard Faculty of Arts and Sciences, and Swarthmore College to offer the first systematic analysis of the use of gender/sex related variables in clinical algorithms across medical specialties. Through the examination of 602 existing clinical algorithms, we document the extent to which gender/sex variables are included in these tools, how they are used, and with what consequences for patient care.
Our analysis identifies a need for greater clarity and accuracy in the use of gender/sex in clinical algorithms, and highlights the importance of including these inputs only when evidence-based, appropriately justified, and systematically re-evaluated over time. This work builds upon a growing body of research attesting to the importance of accurately specifying inputs within clinical algorithms, including ongoing debates in response to evidence indicating that race-based inputs systematically exacerbate racial inequities.
“...It is unclear whether the common practice of using broad gender/sex binary categories...is sufficiently informative and empirically well justified”
Gender/sex inputs are common in clinical algorithms, but their inclusion is often poorly specified or justified
One in six clinical algorithms had at least one input that included gender/sex information, most commonly in binary forms (e.g., “female” vs. “male”, or “exogenous hormone use” vs. “no exogenous hormone use”). None of these tools provided guidance about caring for intersex, non-binary, or transgender patients. Gender/sex information was most often used to allocate “points” directly toward a total score used for interpretation of the tool’s output, but we also found that gender/sex was used to interpret other information as well (for example, different anemia thresholds for males vs. females) (see Figure 1). These uses carried important consequences; across the tools that included gender/sex, preliminary analysis indicated that “tools tended to assign higher diagnostic likelihood, poorer prognosis, and stronger indication for treatment to male patients or patients with characteristics typically associated with male sex…. Treatments favoring male or nonpregnant patients included medical therapy, surgical intervention, hospital admission, and transfusion.”
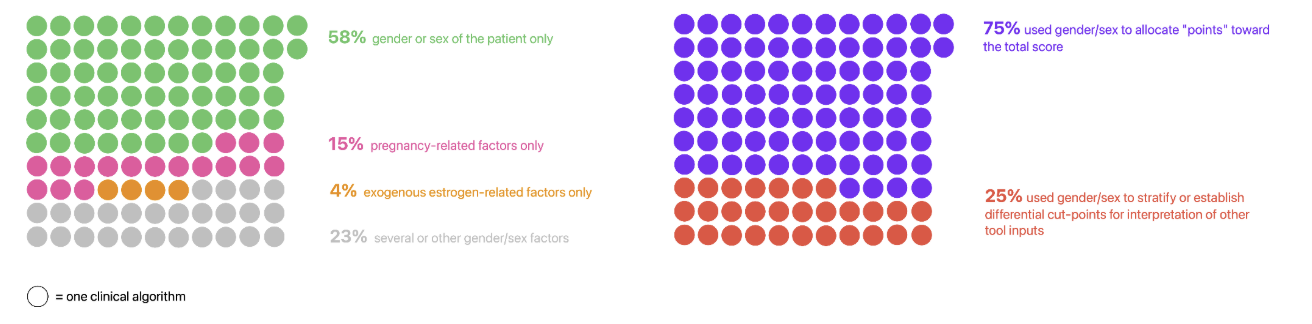
Figure 1: Out of the 602 tools reviewed, 112 (18%) included gender/sex inputs. The panel on the left hand side shows a breakdown of the kind of information recorded by gender/sex inputs, while the panel on the right hand side shows a breakdown of the uses of gender/sex inputs within the tools.
Identifying which aspects of gender/sex are contributing to increased risk or greater likelihood of diagnosis is key to ensuring that clinical algorithms support the delivery of high-quality patient care. However, clinical algorithm developers often provided minimal justification for including gender/sex information in these tools in the first place. Less than half of tools included any substantive biological, clinical, or social justification, with an additional third relying purely on a statistically significant correlation between gender/sex and the outcome of interest. To avoid instances of risk misclassification, we encourage algorithm developers, users, and professional societies to carefully interrogate the clinical relevance of including broad-stroke gender/sex variables in clinical decision-support tools and advocate for operationalizations of such variables informed by etiological clarity as to which specific aspect(s) of gender/sex may shape health risks.
The inclusion of gender/sex inputs is stable over time – but should it be?
We also found that gender/sex inputs in clinical algorithms were rarely updated to include or exclude gender/sex once developed. This relative stability runs counter to increasing evidence over the past fifteen years suggesting that population distributions of gender/sex disparities – and, hence, their (social) determinants – have changed substantially over time for many health outcomes, ranging from cancer mortality to depression. One telling example is the contested inclusion of “female sex” as a risk factor in a tool used for evaluating patients with atrial fibrillation for anticoagulation therapy as a mode of thromboembolic stroke prevention. Patient sex (male/female), still featured in the version of this algorithm recommended by the American Heart Association, was recently removed from the updated tool recommended by professional cardiology societies in Australia, New Zealand, and Europe on the grounds that the inclusion of patient sex affected the tool’s performance over time. For instance, a Finnish study reported that the algorithm specifying patient sex category performed better in 2007-2008, but the algorithm that does not was superior in 2017-2018 – a change that paralleled a reduction in gender/sex disparities in thromboembolic stroke risk, likely itself a reflection of shifts in time-varying gendered risks. These changes suggest that systematic reconsideration and periodic re-evaluation of how and why gender/sex inputs are included in clinical algorithms may be warranted.
“Greater rigor in biologically, clinically, and socially justifying the use and nonuse of gender/sex inputs is warranted, including through systematic, iterative processes to revisit the prognostic necessity of gender/sex inputs over time”
Ultimately, the quality of the outputs from these clinical algorithms – which guide patient care from the primary care clinic to the intensive care unit – relies on the quality of their inputs. By making the inclusion of gender/sex information in clinical algorithms contingent on sound rationales and increasing the clarity, specificity, and accuracy with which they are operationalized, clinicians will be better positioned to provide equitable, high-quality patient care.
Davis, S.H., Danielsen, A.C., Hsiao, I.Y., Albert, K., Delano, M., Shachar, C., Richardson, S.S., Jones, D.S., & Krieger, N. (2026). The extent of gender/sex variables included in clinical algorithms across medical specialties. Health Affairs, 45(7). https://www.healthaffairs.org/doi/10.1377/hlthaff.2025.01772.
STATEMENT OF INTELLECTUAL LABOR
Seetha Davis drafted and revised the blog post. Ann Caroline Danielsen and Sarah Richardson provided feedback and edits.
RECOMMENDED CITATION
Davis, S., Danielsen, A.C., & Richardson, S.S. (2026).“Using gender/sex information to make clinical decisions: How, why, and with what consequences?”. GenderSci Lab Blog. July 7, 2026. https://www.genderscilab.org/blog/using-gender-sex-information-to-make-clinical-decisions-how-why-what